Find your goal below and jump straight to what you need.
Last-minute review
You know the material — you just need clean tables before your next block.
Concepts aren’t clicking
You can define the ligaments but keep missing UWorld questions on them.
NBME question strategy
You want to see exactly how NBME turns this anatomy into clinical vignettes.
Table of Contents
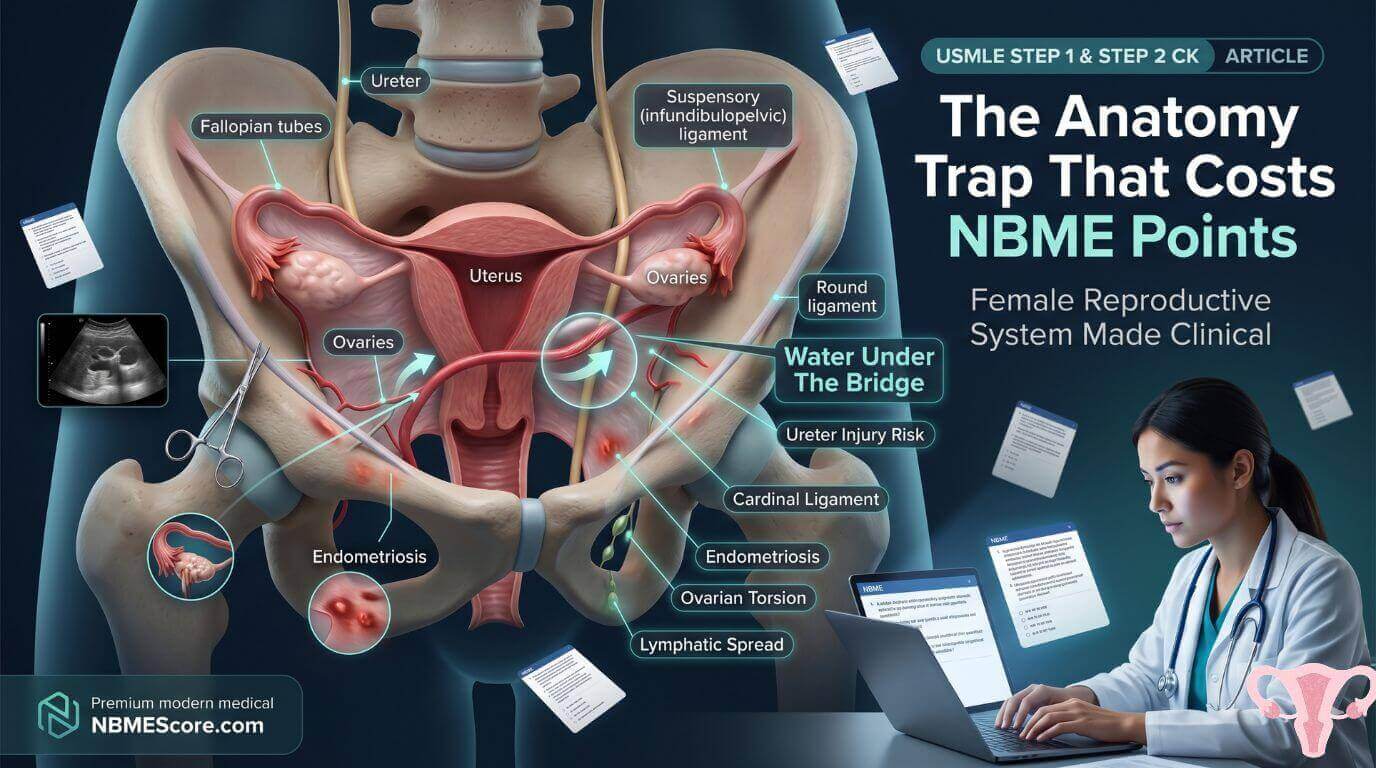
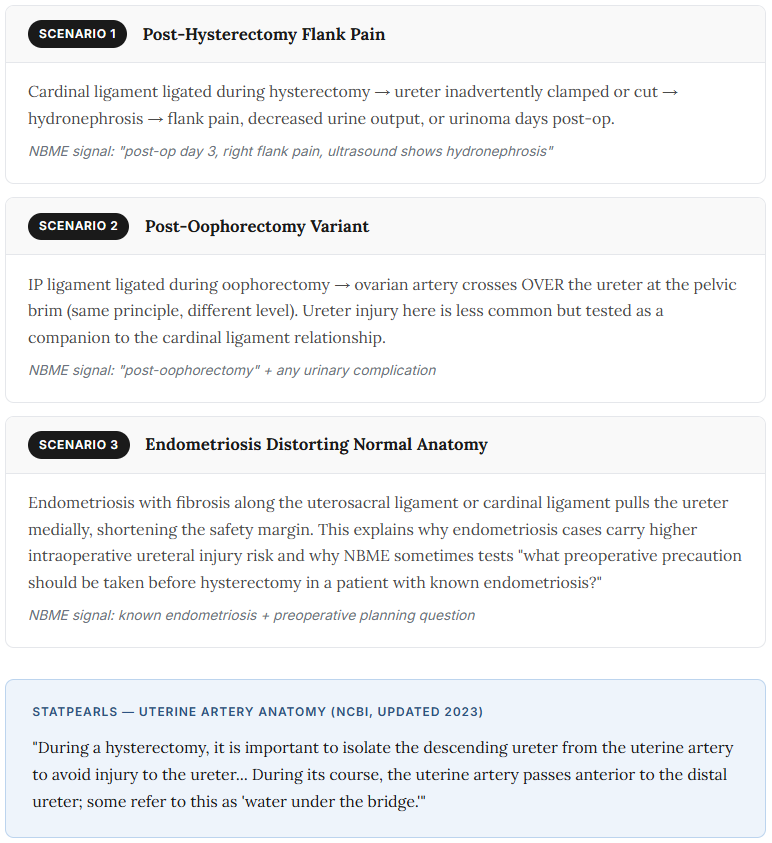
You’re three blocks into an NBME form. A vignette describes a surgeon performing a total abdominal hysterectomy. Post-operatively, the patient develops right flank pain and hydronephrosis on ultrasound. The question: which anatomical structure was most likely inadvertently injured?
Most students who miss this question know exactly what the cardinal ligament is. They can define it, locate it on a diagram, and tell you it connects the cervix to the pelvic sidewall. What they missed was the one piece of information that makes anatomy a clinical question: the ureter passes approximately 2 cm from the uterine cervix, traveling beneath the uterine artery — a relationship so surgically critical that gynecologists call it “water under the bridge.”
This is how NBME uses female reproductive anatomy across both Step 1 and Step 2 CK. Not as a memorization exercise, but as a clinical consequence test. Every structure has a vignette attached to it. This guide maps them both.
Female Reproductive Ligaments: What NBME Tests Beyond the Definition
Every resource lists female reproductive ligaments. None of them explain the pattern NBME uses to test them — which is always consequence, not definition. For each ligament, there are two things worth knowing: what it contains, and what goes wrong when it’s involved in surgery or pathology.
True Ligaments — Actual Connective Tissue
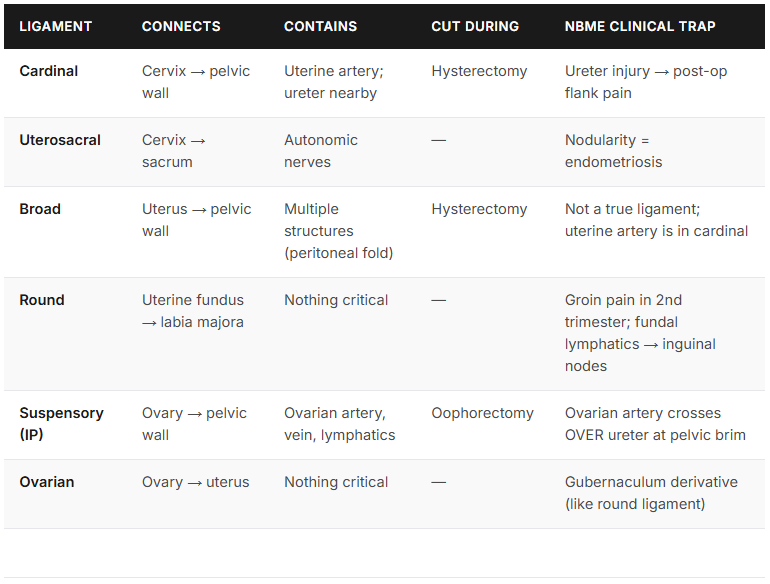
Cardinal Ligament (Mackenrodt’s / Transverse Cervical Ligament)
Connects the cervix and lateral vaginal fornix to the lateral pelvic wall. It is the primary support ligament of the uterus and contains the uterine artery and vein. Inside the cardinal ligament, per StatPearls, the ureter passes approximately 2 cm below the uterine artery — this is the most tested anatomical relationship in pelvic surgery. Surgical injury most commonly occurs in the distal 3 cm of the ureter as it crosses under the uterine vessels within the cardinal ligament before entering the bladder.
Uterosacral Ligament
Connects the posterior cervix to the sacrum. Contains autonomic nerve fibers to the uterus. The NBME clinical significance here is endometriosis — nodularity or tenderness along the uterosacral ligaments on bimanual exam is the specific physical finding that points toward endometriosis, and it explains the fixed, retroverted uterus seen when adhesions form.
Peritoneal Folds — Not True Ligaments
Broad Ligament
A double-layer peritoneal fold extending laterally from the uterus to the pelvic walls. It has three named portions: the mesometrium (uterine portion, largest), mesosalpinx (fallopian tube mesentery), and mesovarium (ovarian attachment). The broad ligament houses the round ligament, fallopian tube, ovarian and uterine vessels, lymphatics, and nerves — but does not itself contain the uterine artery. That artery travels in the cardinal ligament. This is an NBME trap: “the uterine artery travels in the broad ligament” is technically incomplete and occasionally marked wrong depending on how the question is phrased.
Round Ligament
Runs from the uterine fundus through the inguinal canal to the labia majora. It is a remnant of the gubernaculum — embryologically, the same structure that became the ovarian ligament before it interacted with the developing uterus. Contains no major vessels. Its clinical value on USMLE is twofold: round ligament pain in the second trimester (stretching produces sharp groin pain that travels through the inguinal canal), and the fact that lymphatics from the uterine fundus travel with the round ligament through the inguinal canal — the anatomical explanation for why endometrial cancer of the fundus can occasionally present with inguinal lymphadenopathy.
Ovary-Specific Ligaments
Suspensory Ligament of the Ovary (Infundibulopelvic / IP Ligament)
Connects the ovary to the lateral pelvic wall. Contains the ovarian artery (a direct branch of the abdominal aorta), ovarian vein, nerves, and lymphatics. The ovarian artery crosses over the ureter at the pelvic brim — the companion relationship to “water under the bridge” at the cardinal ligament level. The IP ligament is what gets ligated during oophorectomy.
Ovarian Ligament
Connects the ovary to the lateral aspect of the uterus. Like the round ligament, it derives from the gubernaculum. Contains no major vessels. It does not get ligated during oophorectomy — the IP ligament does.
The Ureter Relationships — One Mnemonic, Three Clinical Scenarios
“Water under the bridge” describes the relationship between the uterine artery and the ureter: the artery (water) passes anteriorly and superiorly over the ureter (bridge). StatPearls confirms the uterine artery passes anterior to the distal ureter during its course through the cardinal ligament. The ureter typically lies approximately 2 cm from the uterine cervix — close enough that it is the leading cause of iatrogenic ureteral injury, occurring in 0.1–1.5% for benign hysterectomy, higher for laparoscopic and malignant cases.
What most study guides miss is that this one anatomical relationship generates at least three distinct NBME question types:
Blood Supply: What Step 1 Tests vs. What Step 2 CK Tests
The blood supply questions are completely different at the two exam levels. Understanding which exam is asking which question eliminates a major source of confusion in review.
Step 1 — Origin, Course, Branches
The uterine artery is a branch of the internal iliac (hypogastric) artery. Its ascending branch travels superiorly in the broad ligament and anastomoses with the ovarian artery. Within the myometrium, it branches into arcuate arteries → radial arteries → spiral arteries (supply endometrium, decidua, and placenta) and basal arteries (supply the basal layer, do not shed during menstruation).
The ovarian artery is a direct branch of the abdominal aorta — the same as the testicular artery in males, because both gonads descend from the same embryological location near the aorta. This origin explains the lymphatic drainage pattern (para-aortic nodes) and why both testicular and ovarian tumors bypass pelvic nodes to reach para-aortic nodes directly.
Venous Asymmetry — High-Yield for Step 1
Same as left testicular vein. The acute angle of drainage into the renal vein creates higher venous pressure — clinically relevant for left-sided varicocele equivalents and nutcracker syndrome.
More direct drainage. Right-sided ovarian vein thrombosis can occur in the postpartum period — a rare but tested cause of right-sided flank pain and fever days after delivery.
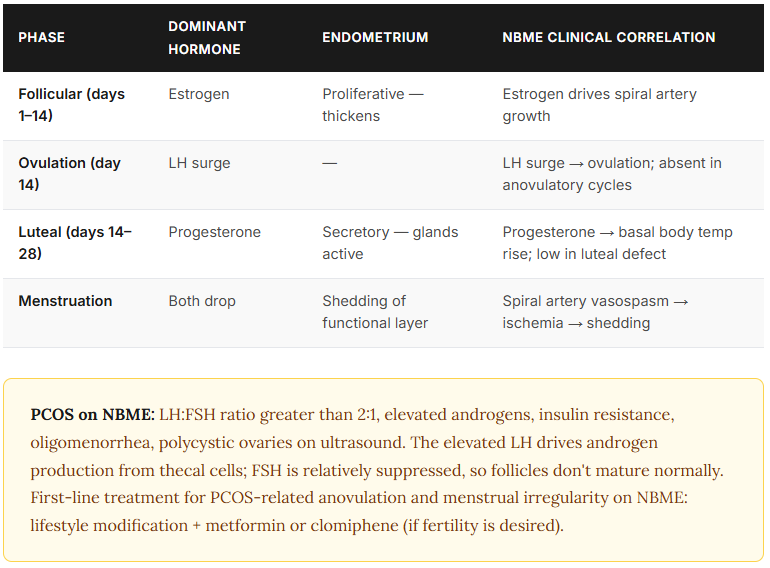
Step 1 — Menstrual Cycle Hormones
The hormone sequence NBME tests most often: FSH rises early → follicle develops → estrogen rises → LH surge (triggered by high estrogen, positive feedback) → ovulation at day 14 → corpus luteum forms → progesterone dominant in luteal phase → if no implantation, corpus luteum regresses → progesterone drops → menstruation.
Step 2 CK — Clinical Consequence of Blood Supply
On Step 2 CK, blood supply questions are clinical. Spiral artery vasospasm is the mechanism of menstruation — the endometrial functional layer is shed when spiral arteries constrict, cutting off blood supply. Uterine artery embolization (UAE) is tested as a fertility-sparing treatment for symptomatic uterine fibroids. Ovarian torsion presents with absent venous and arterial flow on Doppler ultrasound — and the next step is immediate surgical detorsion, not watchful waiting, because prolonged torsion leads to ovarian infarction.
For OB/GYN questions structured as “next best step in management,” see our Step 2 CK next best step framework — the clinical reasoning process is different from anatomy questions.
Lymphatic Drainage: The Cancer Staging Map
Lymphatic drainage questions on USMLE are never about anatomy for its own sake. They explain where cancer spreads — and understanding that each drainage pathway follows the blood supply is the organizing principle that makes the whole map memorizable.
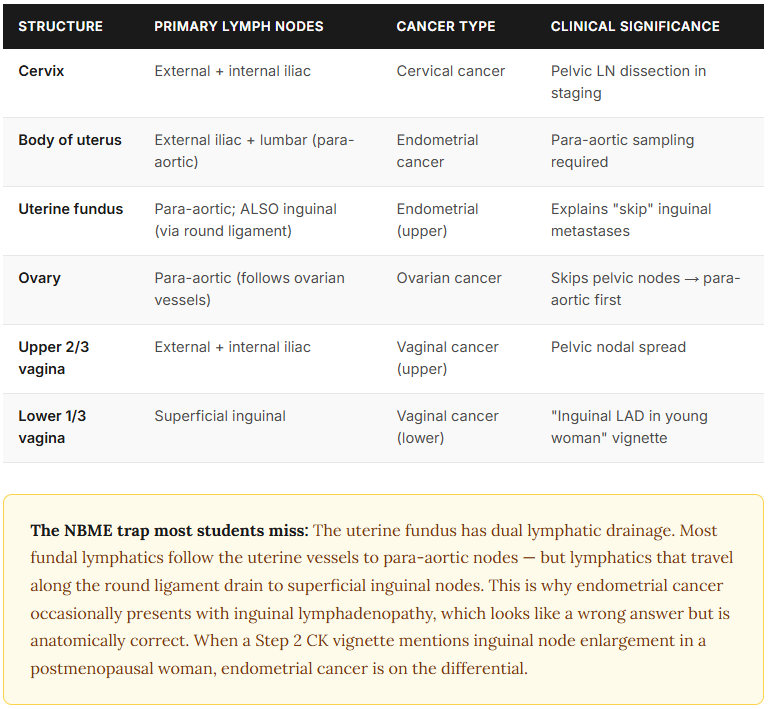
Lymphatics follow blood supply — that’s the principle that makes the whole map learnable. Ovarian blood comes from the aorta, so ovarian lymphatics drain to para-aortic nodes. Uterine blood comes from the internal iliac, so uterine lymphatics drain to pelvic nodes. The round ligament pathway is the exception NBME consistently tests because it looks counterintuitive until you know the anatomy behind it.
If your NBME scores plateau in the OB/GYN subject breakdown, targeted OB/GYN CMS forms are the most efficient way to identify whether anatomy-based clinical reasoning is the specific gap.
Anatomy of Uterus and Ovaries: The Layers and the Questions They Generate
Uterine Wall Layers
From outside in: perimetrium (outer serosa), myometrium (thick smooth muscle layer — contracts during labor and menstruation), endometrium (inner glandular layer — divided into a functional layer that sheds each cycle and a basal layer that regenerates).
The myometrium-endometrium distinction generates one of the most testable diagnoses in gynecology: adenomyosis is endometrial glands found within the myometrium. The clinical picture is a uniformly enlarged, boggy, tender uterus in a multiparous woman with heavy periods and dysmenorrhea. Compare this to fibroids: uterine leiomyomas produce asymmetric, firm, irregular uterine enlargement. The uniformly enlarged tender uterus = adenomyosis; the irregular nodular uterus = fibroids. NBME uses this distinction consistently.
Pouch of Douglas (Rectouterine Pouch)
The lowest point of the peritoneal cavity in females — located between the uterus anteriorly and the rectum posteriorly. This anatomical position makes it the collection point for blood, pus, or ascites that accumulates in the pelvis. Culdocentesis — aspiration of fluid through the posterior vaginal fornix — accesses this space directly and was historically used to diagnose ectopic pregnancy (blood in the cul-de-sac) or PID (purulent fluid). On NBME, the posterior fornix + needle aspiration + bloody fluid = ruptured ectopic pregnancy until proven otherwise.
Ovarian Structure
The ovarian cortex contains the follicles, corpus luteum, and corpus albicans. The medulla contains the blood vessels, lymphatics, and nerves that enter at the hilum via the mesovarium. Ovarian torsion compromises both arterial inflow and venous outflow simultaneously — explaining why it presents with sudden severe unilateral pelvic pain, nausea, and vomiting, and why Doppler showing absent flow is the key imaging finding.
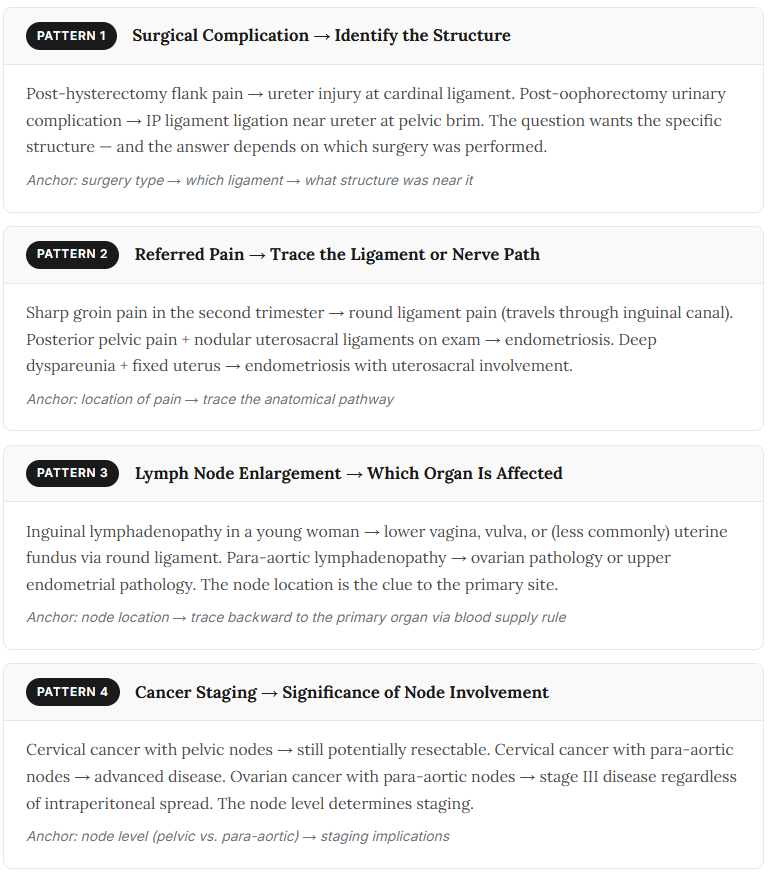
Five NBME Vignette Patterns from Female Reproductive Anatomy
These are the specific clinical scenarios NBME builds from this anatomy. Recognizing the pattern type before reading the answer choices changes how you approach the question.
Müllerian Development: The Embryology NBME Tests Consistently
Female Reproductive System USMLE anatomy questions on Step 1 frequently reach back one layer — to where these structures came from. The Müllerian (paramesonephric) duct system is the embryological origin of most of the female reproductive tract, and NBME tests both its normal development and what happens when it goes wrong.
In females, Müllerian ducts develop and fuse in the midline to form the uterus and upper vagina. The unfused portions become the fallopian tubes. Incomplete fusion → bicornuate uterus (recurrent miscarriages, preterm labor). Complete agenesis (MRKH syndrome) → no uterus or upper vagina, normal 46,XX karyotype, normal secondary sex characteristics.
In females without testosterone, mesonephric ducts degenerate. Vestiges can persist as Gartner’s duct cyst — a benign cyst found in the anterolateral vaginal wall. NBME tests this as the structure that should have degenerated. In males, the same ducts become the epididymis, vas deferens, and seminal vesicles.
Two additional Müllerian development concepts NBME tests on Step 1: DES exposure in utero (daughters of women who took diethylstilbestrol have T-shaped uterus abnormalities and increased ectopic pregnancy risk — a historical teratogen question) and hydrometrocolpos (imperforate hymen → accumulation of secretions in vagina and uterus → midline pelvic mass in a newborn girl).
FAQ: Female Reproductive System USMLE
Que. An NBME question said the uterine artery was “in the broad ligament” — is that wrong?
Ans. It depends on how precise the question is being. The uterine artery technically travels in the cardinal ligament, but the cardinal ligament forms the base of the broad ligament — so NBME sometimes uses “broad ligament” loosely to mean the entire parametrial region. The precise answer for Step 1 anatomy questions is the cardinal ligament. For Step 2 CK management questions, the distinction usually doesn’t change the answer. Know both, but default to cardinal ligament for anatomical precision questions.
Que. Does the round ligament contain vessels I need to know?
Ans. Not for surgical purposes — no major vessels. It’s clinically relevant for two reasons: round ligament pain in pregnancy (the ligament stretches as the uterus grows, producing sharp groin pain that travels through the inguinal canal), and the fact that lymphatics from the uterine fundus travel with it through the inguinal canal. The second point explains how endometrial cancer of the fundus can occasionally spread to inguinal nodes instead of the expected para-aortic nodes — a pattern that looks wrong until you trace the anatomy.
Que. What’s the difference between the ovarian ligament and the suspensory ligament?
Ans. Ovarian ligament: connects ovary to uterus, contains nothing critical, gubernaculum derivative. Suspensory (infundibulopelvic / IP) ligament: connects ovary to the lateral pelvic wall, contains the ovarian artery, vein, lymphatics, and nerves. The IP ligament is what gets ligated during oophorectomy. The ovarian ligament stays behind. On NBME, “structure ligated during oophorectomy” = IP ligament, not ovarian ligament.
Que. Which lymph nodes does ovarian cancer spread to first?
Ans. Para-aortic nodes — the same initial drainage as testicular cancer — because the ovarian blood supply derives directly from the abdominal aorta and lymphatics follow blood supply. Ovarian cancer characteristically skips pelvic nodes and involves para-aortic nodes first. This explains the staging implication: para-aortic node involvement in ovarian cancer represents stage III disease, and it’s why para-aortic lymph node sampling is part of complete surgical staging.
Que. Why does adenomyosis produce a uniformly enlarged uterus while fibroids produce an irregular one?
Ans. Adenomyosis is diffuse infiltration of endometrial glands into the myometrium throughout the uterine wall — the enlargement is uniform because the entire myometrium is involved. Fibroids (leiomyomas) are discrete smooth muscle tumors that grow in distinct locations (submucosal, intramural, subserosal), creating focal bulges that make the uterus feel nodular and asymmetric. On NBME, the uniform boggy tender uterus in a multiparous woman = adenomyosis; the irregular nodular non-tender uterus = fibroids.
Que. What is culdocentesis and when does NBME test it?
Ans. Culdocentesis is aspiration of fluid from the rectouterine pouch (Pouch of Douglas) through a needle inserted through the posterior vaginal fornix. It’s tested in the context of suspected ruptured ectopic pregnancy — bloody non-clotting fluid aspirated from the cul-de-sac is a positive finding. In the era of transvaginal ultrasound, culdocentesis is rarely done clinically, but it appears on NBME in historical or resource-limited settings. Knowing that the posterior fornix is the access point and the pouch of Douglas is the lowest peritoneal collection point is the anatomy underlying the procedure.
Female reproductive anatomy becomes manageable for USMLE once you stop treating it as a list of structures to memorize and start treating it as a map of clinical consequences. Every ligament has a surgery associated with it. Every lymphatic pathway has a cancer that follows it. Every blood supply variant has a clinical presentation that results when something goes wrong.
The students who score well in this category on their NBME forms aren’t the ones who drew the most detailed anatomy diagrams. They’re the ones who read “post-hysterectomy hydronephrosis” and immediately trace it: cardinal ligament → uterine artery → ureter crossing beneath it → two centimeters from the cervix. Track your subject-level performance on your NBME Step 2 CK score breakdown.